Phase 1: Exploration
Identifying human factors and environmental factors before implementing acupuncture or acupressure in a hospital setting.
Prior to implementation, it is necessary to establish a good understanding of the human factors and environmental factors within which the implementation will happen. Factors to be considered are:
- Does an internal need for change exist?
- What intervention types are available?
- Who should be on the implementation team?
- What are staff perspectives on the proposed changes?
- What are patient requirements?
- Is funding necessary and available?
- Is the organisation ready for change?
Identify Internal Needs
Using PONV (postoperative nausea and vomiting) as example:
How is PONV prevented and managed locally?
- Review hospital practice guidelines for PONV management
Is PONV incidence charted?
- Check observation charts in Recovery, ward, and pre-discharge phases
- Verify documentation across all care settings
What is current PONV incidence and rescue antiemetic usage?
- Track current incident rates
- Monitor rescue medication administration
- Note: "rescue anti-emetic use is not equivalent to PONV"
- Resource: PONV study data extraction template provided
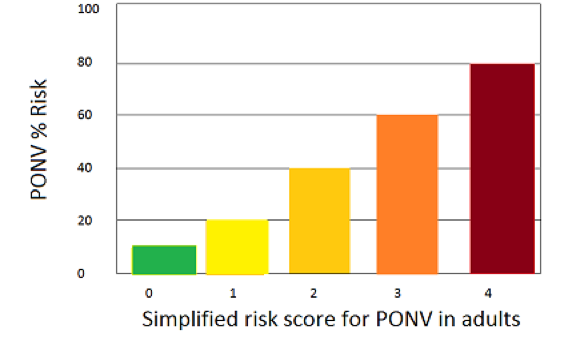
Is PONV risk assessed?
"PONV risk assessment is the first recommendation for PONV management" (Gan 2014). Four primary risk factors identified:
- Female gender
- Non-smoker status
- Previous PONV or motion sickness history
- Post-operative opioid use
Risk increases 20% per additional factor (Apfel et al., 1999). Patient self-assessment checklist available.
Intervention
Compare the main acupuncture and acupressure modalities below. Expand any row for detailed effectiveness data, advantages, disadvantages, and implementation notes recovered from the legacy POPA4Ease site.

| Modality | Invasiveness | Evidence Snapshot | Cost / Equipment | Training | Details |
|---|---|---|---|---|---|
| Manual Acupressure | Non-invasive | Practical low-cost option with reduced nausea and vomiting in the legacy source. | No equipment | Low | View detailsEffectiveness
Advantages
Disadvantages
|
| Transcutaneous Electrostimulation | Non-invasive | Strong non-invasive option with adjustable stimulation and extended-use potential. | $40-$200 equipment | Moderate | View detailsEffectiveness
Advantages
Disadvantages
|
| Auricular Acupuncture | Needle-based | Procedure-specific evidence in gynaecological surgery and laparoscopic cholecystectomy. | Few cents per needle or bead | Moderate | View detailsEffectiveness
Advantages
Disadvantages
|
| Body Acupuncture | Needle-based | Direct body acupuncture with clear reductions in nausea, vomiting, and total PONV. | $0.05 per needle | Moderate | View detailsEffectiveness
Advantages
Disadvantages
|
| Electroacupuncture | Needle-based | Body acupuncture with adjustable electrical stimulus and reusable stimulation units. | $200-$800 equipment plus needles | Moderate | View detailsEffectiveness
Advantages
Disadvantages
|
| Acupressure Band or Patch | Non-invasive | Improves nausea, vomiting, and rescue antiemetic use with low training burden. | About $5 AUD | Low | View detailsEffectiveness
Advantages
Disadvantages
|
| PC6 Acupoint Stimulation (All Modalities) | Mixed | Strong pooled effect across modalities with mild transient side effects. | Varies by modality | Moderate | View detailsEffectiveness
Advantages
Disadvantages
|
The Team
The Implementation Team
Team composition should include:
Opinion Leaders / Facilitators
"Individuals in an organization who have formal or informal influence on attitudes and beliefs regarding intervention implementation."
Champions
Individuals who "drive through an implementation, overcoming indifference or resistance."
External Change Agents
External individuals who "formally influence or facilitate intervention decisions."
Key principle: Early users should share professional, educational, cultural, or socioeconomic backgrounds with leadership for successful implementation.
Staff
Staff Groups Requiring Involvement
- Anaesthetists
- Nurses
- Midwives
- Gynaecologists / Obstetricians
- Surgeons
- Administrative clerks
- Interpreters
USA Survey Results (Faircloth, 2014)
Respondents: 292 from 1,728 anaesthesia staff across 96 departments.
Composition: 54% anaesthesiologists, 44% nurses, 2% aides.
- Prior use with positive outcomes: 27%
- Willing to consider use: 54%
- Willing to pursue education: 74%
Main barriers:
- "Lack of scientific evidence" (79%)
- "Unavailability of credentialed providers" (71%)
- "Lack of equipment" (49%)
Time concern: Only 38% viewed acupuncture as too time-consuming.
Australian Hospital Survey Results
Respondents: 165 doctors, nurses, midwives, obstetricians (Zheng et al., reference to be confirmed).
- Believed effective for PONV: 42%
- Would encourage patients after education: 81%
- Wanted further education: 88%
Australian General Practice Context
- National survey of 544 GPs: ~85% considered acupuncture effective and safe for primary care (Cohen et al., 2005)
- GP referral rate: 80% have referred patients (Wardle et al., 2013)
- Medical school integration: Some Australian schools teach acupuncture as electives
Readiness for Change
Organizational Readiness Assessment
Tool: Modified Checklist to Assess Organization Readiness (CARI) (Barwick, 2011)
Evaluates:
- System readiness
- Senior leadership support
- Staff capability
- Implementation plan maturity
- Training requirements
Scoring: 8 categories, each worth 20 points (160 points total). Readiness threshold: 80% overall.

Funding
Cost and Funding Considerations
Cost Assessment Framework (Myle, 2016):
Costs to Track:
- Device cost per patient
- Staff time for intervention delivery
- Staff time for intervention monitoring
- Prevention antiemetic medications and costs
- Rescue antiemetic medications and costs
- Intra-operative and post-operative pain medications and costs
Assessment Methods:
- Track intervention delivery time (minutes)
- Document medication type and dosage
- Calculate pharmaceutical costs
- Calculate device costs
- Compare cost-effectiveness against alternatives
Cost Comparison
- Acupressure wristbands: ~$8–$15 AUD per unit (single ~$8, pair ~$15)
- Acupuncture needles: ~$0.10–$0.20 per needle (~$0.60–$1.20 per treatment)
- Electroacupressure units: $40–$200
- Electroacupuncture units: $200–$800
Patient
Patient Perspectives
Patient Survey Results (Weeks et al., 2017):
Sample: 160 surgical patients (Australian).
- Pre-education willingness: 65% would use acupuncture for PONV
- Baseline knowledge: Only 15% knew acupuncture could treat nausea/vomiting
- Post-education willingness: 87% (22-percentage-point increase)
PONV Management Guideline Recommendation: Interventions should consider patient preferences when selecting treatment approaches.
Phase 1 Resources
- PONV risk self-assessment checklist
- PONV data extraction template (Excel) — coming soon
- Modified CARI readiness checklist — coming soon
- Sample staff survey questions — coming soon
- Patient survey results and template — coming soon
Last reviewed: April 2026